Hemodialysis treatment
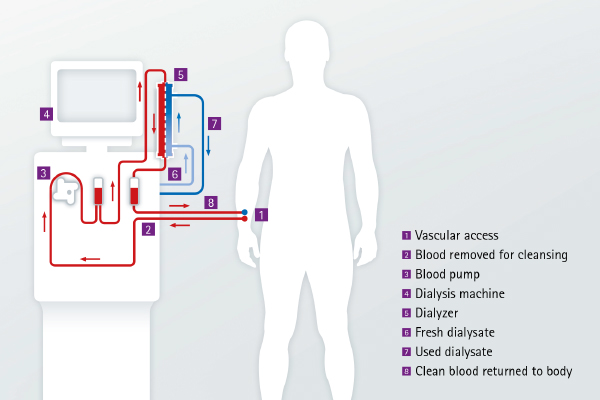
Hemodialysis cleans your blood using a special filter known as a dialyzer. Those patients who opt for this form of treatment undergo a minor surgical procedure to create a AV fistula that provides easier access to the bloodstream for the staff and makes it more convenient. It only takes a few days for the fistula to heal, but we have to give it several weeks to mature, which means to become fully functional and ready to be used. From the AV fistula, blood can readily be channeled to and from the dialyzer through a system of tubes, called bloodlines.
During treatment, the blood is cleaned in the dialyzer. The cleaning process does not cause any pain and many patients will experience improvement of their condition especially in the beginning of dialysis treatment. However, if you feel unwell or uncomfortable during treatment, you should tell the staff, who will help you. Depending on your medical history, you will usually undergo hemodialysis three times a week with an average session time of 4-5 hours each treatment.
Hemodialysis is the most common method used to treat chronic kidney failure. It is mostly performed at a renal care center under the supervision of experienced and well-trained medical staff.
Advantages
- You are completely free on the days between dialysis sessions and need not worry about treatment.
- Thanks to modern technology, blood purification has become gentler and more effective. Treatment usually takes place in a renal care center.
Frequently asked questions: hemodialysis
Varför behöver jag bloddialys?
Orsaken till att du behöver dialysbehandling är att du har njursvikt vilket innebär att dina njurar fungerar dåligt eller inte alls. Njurarna är normalt kroppens filter där uringifter samt överskott på salter och vatten filtreras bort. Hemodialys är en behandling som avlägsnar toxiner så som Urea och Kreatenin från kroppen.
Hur utförs hemodislys?
Under en hemodialys förs blod ut från kroppen och filtreras via ett dialysfilter (dialysator) innan det förs tillbaks till din kropp. Filtret består av flera hundratals små rör (kapillärer) i vilka blodet passerar. Dessa rör har tusentals små hål som tillåter uringifter och lösta ämnen samt vatten att passera. Detta spolas ut via dialysmaskinens avlopp.
På utsidan av de små rören finns dialysvätska (dialysat) som består av speciellt renat vatten och tillsatta salter. Kompositionen av denna vätska är ordinerad av en läkare för att passa din kropp och behov. Maskinen blandar det renade vattnet med saltkoncentrat samt bikarbonat och kontrollerar blandningen innan den leds ut till filtret.
Hur renar filtret mitt blod?
Som tidigare beskrivits har dialysfiltret två delar, en blodsida och en dialysatsida som är avskilda från varandra. Blod och dialysat blandas inte.
Små partiklar såsom uringifter, överskottssalter och vatten kan passera genom de små hålen i rören. Större partiklar såsom blodkroppar och äggviteämnen (proteiner) kan inte passera och behålls i blodet. Ordinationen av dialysvätska och flöden är personliga och ordineras av vårdpersonalen.
Vad tas bort under en dialysbehandling?
Vi försöker att efterlikna kroppens egna funktion genom att ta bort de ämnen som njuren normalt filtrera bort såsom Urea och Kreatenin. Vissa salter utsöndras också via njurarana, till exempelvis Natrium och Kalium och överskott av dessa tas också bort. Dialysbehandlingen strävar att utjämna skillnader i saltbalansen så har du brist på Natrium eller Kalcium så passerar dessa in i blodet från dialysatet. Ett stort problem vid dialysbehandling kan vara att du samlar på dig överskottsvätska som du normalt skulle ha kissat bort. En viktig del av dialysbehandlingen är att ta bort denna vätska. Både höga halter Natrium och överskottsvätska kan påverka blodtrycket så att det stiger. Höga halter Kalium kan påverka ditt välbefinnande och orsaka hur ditt hjärta arbetar.
Hur mycket blod renas under en behandling?
Behandlingens kvalitet beror på hur mycket blod som kan tas ut från kroppen. Detta beror på blodkärlsaccessen. Vi eftersträvar så högt blodflöde som är möjligt, vanligtvis mellan 200-350 ml/min. Blodpumpen på dialysmaskinen sköter detta flöde. För att undvika att blodet koagulerar och andra komplikationer försöker vi att ha en sådan liten volym av blod utanför kroppen som möjligt.
Vilka typer av blodkärlsaccess finns det?
- Vi skiljer vanligtvis på Fistel/ Graft och Central Dialyskateter
Hur lång dialysbehandling behöver jag och hur ofta?
Detta beror mycket på:
- Vilken restfunktion du dina njurar har
- Hur mycket vätska du samlar på dig mellan behandlingarna
- Hur mycket uringifter du har
- Kroppsstorlek och vikt
- Vilken typ av dialysator och behandling du har
Behandlande läkare väger in dessa parametrar och ordinerar den behandling som passar dig. Även blodflöde, dialysatflöde och vilken typ av koncentrat som du behöver för att nå en korrekt dialysdos. Rätt dialysdos och en aktiv övervakning av din torrvikt (överskottsvätska) hjälper dig till ett bra välbefinnande.
Vad gör dialysmaskinen under en behandling?
Dialysmaskinen är designad för att ge en säker och effektiv behandling. Den kan liknas med en stor dator med en blodpump. Den utför och kontrollerar de processer som behövs för en bra behandling så som blod- och dialysatflöde, blodtrycket, blandningen av dialysatet och andra vitala parametrar.
Vad händer när jag kommer för en dialysbehandling?
Varje dialysavdelning har en speciell rutin för att ta hand om dig när du kommer för din behandling. Dessa rutiner kan se lite olika ut men det finns stora likheter. Du får väga dig och ditt blodtryck mäts. Detta är en viktig del för att bedöma hur mycket överskottsvätska som skall tas bort. Det är viktigt att du talar om hur du mår och hur du mått sedan din senaste behandling. Detta är en viktig del i att bedöma ditt allmäntillstånd. Vissa dagar tas det blodprover. Sedan ansluts du till dialysmaskinen och behandlingen börjar.
Vad händer under en dialysbehandling?
När behandlingen har startat så är det mycket upp till dig vad du vill och kan sysselsätta sig med så länge du kommer ihåg att du är ansluten till en dialysmaskin.
Du kan läsa, prata med andra patienter, se på tv/film, lyssna på radio, lösa korsord eller använda dator/surfplatta. Vissa avdelningar har träningsutrustning som du kan använda under behandlingen.
Personalen kommer att kontrollera ditt blodtryck och hur du mår regelbundet. Passa på att fråga personalen om din sjukdom och behandling.
Varför blir det ett larm på dialysmaskinen?
En av maskinens funktioner är att kontrollera att alla processer fungerar. Maskinen har inställda larmgränser för många parametrar och hamnar värdena utanför dessa gränser ger maskinen larm och processen stannar. Detta för att ge dig en säker behandling. Maskinen larmar även när det är dags att avsluta behandlingen. Fråga personalen varför maskinen har utlöst ett larm.
Kommer jag att må bättre efter min behandling?
Dialysbehandlingen ska få dig att må bättre såvida du inte är sjuk av något annat än din njursvikt. Ibland kan du känna dig trött och slut efter en behandling men kommer förmodligen att känna dig piggare dagen efter. Vissa personer behöver ”vänja” sig med behandlingen, andra mår bra med det samma. Detta är väldigt individuellt och kan också variera över tid. Prata med vårdpersonalen om du inte mår bra.
Finns det några biverkningar eller komplikationer av behandlingen?
Det finns inga direkta biverkningar av behandlingen men du kan råka ut för några komplikationer. Den vanligaste komplikationen är blodtrycksfall och benkramper. Detta beror oftast på för mycket vätska har avlägsnats för snabbt. Det kan vara så att ditt blodtryck sjunker även fast du har överskottsvätska i kroppen. Det kan ibland vara väldigt svårt att avgöra hur mycket vätska som kan avlägsnas på kort tid. Det är därför väldigt viktigt att du lyssnar på vårdpersonalen när det gäller vätskedragning och restriktion att dricka vatten mellan behandlingarna. Yrsel och illamående är också valiga symtom på lågt blodtryck. Det kan också vara att du har en felaktig blodtrycksmedicinering eller tar dessa läkemedel för nära behandlingen. Prata med vårdpersonalen.
Vad är min uppgift som patient?
På dialysavdelningen:
- Prata med personalen och redogör för eventuella problem
- Tvätta händerna före och efter behandlingen med tvål och vatten. Använd handsprit
- Informera om du mår dåligt under behandlingen
- Ta del och lär dig om din sjukdom och behandling. Det tjänar alla på
Hemma:
- Följ kost- och vätskeråden du fått
- Ta dina läkemedel enligt ordination, även de sk fosfatbindarna
- Försök att vara aktiv, även den minsta träningen kan öka välbefinnandet.
Vad hander när dialysen tar slut?
När behandlingstid och/eller vätskeborttagningsmål uppnåtts ger maskinen larm. Det blod som då finns i blodslangar och filter återges till dig. Har du en dialyskateter spolas den fri från blod och ett medel för att förhindra koagulation tillsätts och den tillsluts med korkar. Därefter packas den in enligt avdelningens rutiner.
Har du fistel eller graft så tas nålarna ut och blödningen stoppas med ett lätt tryck. Ett plåster eller dylikt appliceras.
Blodtrycket kontrolleras. När personalen har kollat att blödningen från kärlaccessen har stoppat och blodtrycket är inom rimliga gränser får du gå hem om inget annat planerats. Meddela personalen om du mår dåligt.
Vascular access
For dialysis to work properly it needs to create a way to take blood from your body, pass it through the dialyzer, where it is cleaned and then returned safely. Before starting your first HD treatment, an access to your bloodstream has to be prepared. This vascular access allows your blood to be easily taken from a vein in order to flow through the bloodlines to the dialyzer and back through bloodlines into the body. Therefore, such an access has to be surgically created in the arm, leg or near the collarbone. There are three main types of vascular access for hemodialysis treatment: The AV fistula, the vascular access graft as well as the central venous catheter.
Watch carefully for signs of infection: redness, swelling, pain, high pulse rate and fever. If you notice any of these signs, contact your renal care center immediately.
Vascular access for hemodialysis (HD)
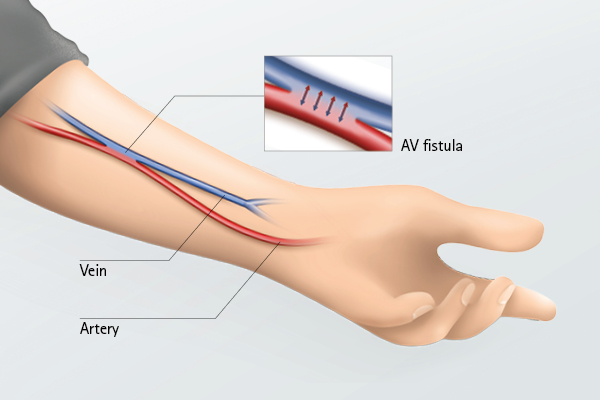
The AV fistula
For hemodialysis, good vascular access is critical to being able to carry out dialysis treatment. It involves the use of blood vessels, which are often not easily accessible or have too little pressure. Therefore, many patients have a vascular connection, also known as AV fistula, placed between the artery and vein of the forearm by means of a surgical procedure. This is the most common method used for vascular access.
AV fistula puncture
Since an AV fistula puncture is an invasive procedure, all the usual pre-operative hygiene measures are adhered to. This is something that dialysis staff (physicians or nurses) are fully trained for and pay close attention to. Dialysis patients should also take care of their hygiene, because they are especially vulnerable to infections due to their disease and reduced resistance. First the AV fistula arm is washed and then cleaned using a disinfectant. The dialysis staff will use gloves and complete the process using strict infection control practices. Here, the standardized hygiene rules are adhered to by the dialysis staff.
Caring for the AV fistula
If you have had a new AV fistula created, you may be asked to carry out some exercises to help the AV fistula develop and mature. This ‘maturation process’ takes about 6-8 weeks. Small softballs developed especially for AV fistula training are best suited for this. You take the balls in your hand and squeeze them in a pumping motion. You also learn to pay attention to the thrill of the AV fistula each day. The thrill is a sign of the blood flow in the AV fistula. You can feel the thrill with your hand. Some patients also use a stethoscope to listen to the so-called bruit. Wound care and changing dressings regularly are the be-all and end-all of caring for an AV fistula. The AV fistula arm can be washed normally after 12-24 hours. In the context of general personal hygiene, you may also apply cream to it using ointment that is easily absorbable. For the prevention of possible complications (such as AV fistula infections), intact skin with good protection is very important.
Vascular access graft
A graft is a small piece of plastic inserted between an artery and a vein in the arm or thigh. If a patient’s veins are too small or weak for an AV fistula to be created, a synthetic graft (made from synthetic material) may be used to form a connection between an artery and a vein. It is placed under the skin like a natural vein. Compared with fistulas, grafts tend to have more problems with clotting or infection and need to be replaced sooner, but a well cared for graft can last for years. The graft as well as the AV fistula lie beneath the surface of the skin.
Central venous catheter
A central venous catheter is a plastic tube placed into a central vein in the neck or chest by a doctor. Sometimes it is not possible to wait until an AV fistula is ready before starting dialysis; that is when a central venous catheter is needed. Temporary catheters are held in place with stitches. Permanent catheters, intended for long-term use, may be held in place by a special cuff under the skin and a few stitches. Catheters can clog, become infected, or cause narrowing of the veins in which they are placed. With good care, a catheter can be a helpful ‘bridge’ while your fistula or graft is healing or can allow you to have dialysis when other forms of vascular access are not available. As catheters are prone to infections, it is highly recommended that the following principles are considered: It is very important to always keep your catheter clean and dry. This means you must not swim, shower or bath with the catheter. Watch for signs of infection: Redness, swelling, pain, high pulse or fever. Call your renal care center right away if you notice any of these signs. Never use scissors or other sharp objects near or around your catheter for any reason.
Frequently asked questions: vascular access
What types of vascular access are there?
The options of vascular access are:
- An Arterio-venous fistula (AV fistula)
- An Arterio-venous graft (AV graft)
- A Central venous catheter
What is an arterio-venous fistula?
A fistula is the most common type of dialysis access. Creating a fistula involves a small operation on the wrist or arm to join together a vein and an artery. The operation takes about an hour. It is usually carried out under local anesthetic and you will spend part of the day in hospital. Joining a vein to an artery creates a faster and more turbulent flow of blood through the vein. This makes the vein thicker and it gets bigger. Eventually, it becomes visible under the skin, looking a bit like a large varicose vein. When you touch it you can feel a “buzz”. This sensation is very important, because it means that the fistula is working properly. You should check your fistula every day and if it ever stops working, contact the hospital immediately.
What is an aterio-venous graft?
A graft is a small piece of plastic inserted between an artery and a vein in your arm or thigh. A small proportion of people have to have a graft if their own veins are not accessible or not strong enough for a fistula. The graft is placed close to the surface of the skin for easier needling.
What is a central venous catheter?
A catheter is used when, for some reason, a fistula is not possible. It is a permanent device and will hopefully last as long as you need it. It involves inserting and securing a soft plastic tube (catheter) about the thickness of a pencil into a large vein in the base of your neck. About six inches of the tube protrudes from your skin and a dressing is placed over the site where it enters your skin. The dressing should be kept clean and dry and extra care is needed when bathing and washing your hair. The tube is easily covered by clothing.
How does my fistula/graft work during dialysis?
During dialysis, two needles are placed into the fistula. One needle will remove the blood so it can be cleaned. The other needle will return filtered blood to the body. The needles are attached by plastic tubing to a special filter called a dialyzer. A pump pushes the blood through the dialyzer. Blood passes on one side of the filter, and solution made by the dialysis machine passes on the other side. The blood does not mix with the solution. Instead, the solution pulls extra fluid and waste out of the blood by a process called dialysis. The "clean" blood returns through the plastic tube. It passes back into the patient's body through the second needle.
How long can an arterio-venous fistula last?
Once the fistula has developed, it can last a very long time. Some patients have a fistula that is still working after 30 years! However, if you are elderly when your fistula is created or if you suffer from other medical conditions such as diabetes, the fistula may not last that long. That said, a fistula or graft is still the best possible option for hemodialysis access because:
- The risk of infection is lower than with a catheter.
- It is less likely to clot.
- It allows for a greater blood flow during dialysis. This makes dialysis more effective.
- A fistula usually has a longer “life” than a graft, and both typically last longer than a catheter.
What are the advantages and disadvantages of each type of access?
Fistula
Pros
- Lasts longer
- Less infection risk
- Good blood flow
- Less likely to clot and become obstructed
Cons
- Takes time to develop after surgery
- Needles are inserted to connect for dialysis
Graft
Pros
- Lasts longer than catheter
- Good blood flow
Cons
- Takes time to develop after surgery
- Needles are inserted to connect for dialysis
- More risk of infection than a fistula
Catheter
Pros
- Can be used straight away
- No needles required for dialysis
Cons
- Higher infection risk than a fistula or graft
- Can clot and become obstructed
- Care needed when bathing or showering
How do I care for my fistula or graft at home?
Check that the fistula is working every day by feeling over the area and by listening to it close to your ear. Your nurse or doctor will show you how to do this. Keep your fistula arm clean and wash it every day. Your nurse will be able to give you advice on the best type of soap to use. Watch for signs of infection. These may be tenderness, swelling or redness over the fistula. You may also have a fever. If you think the fistula has stopped working or that you have an infection, immediately contact the dialysis center for advice. Avoid wearing tight clothing or a wristwatch on the access arm. Avoid having your blood pressure taken on the arm with the fistula. Avoid having blood samples taken from the arm with the fistula (except during HD treatment or with the renal unit's approval). Avoid sleeping on the fistula arm. Avoid carrying heavy shopping bags on the fistula arm.
Do I need to do anything special with my fistula or graft on my dialysis days?
Always wash your access arm before each dialysis treatment. Don’t touch the skin around your access after the nurse has cleaned your arm in preparation to inserting your needles. Don’t cough or sneeze on the access site during dialysis. When your needles have been removed, apply only gentle pressure to stop bleeding. And press only where the needle has been. When you get home, don’t scratch around the needles sites and don’t pick off the scabs.
What should I do if my fistula/graft stops working when I am at home?
If you check your fistula and think you cannot hear or feel the blood going through the fistula, it may have clotted or stopped working. Phone the dialysis center immediately for advice. It may be possible to “rescue” the fistula. Don’t wait until “tomorrow because that is your usual dialysis day” – it will be too late.



